精读笔记
Problem Setting
这篇论文真正处理的是 graph/landmark-based cardiac segmentation 的 temporal identity problem,而不是单纯提升 segmentation accuracy。Mask-HybridGNet 类方法已经能通过固定拓扑图和 Chamfer supervision 学到跨个体的隐式 anatomical correspondence,但它逐帧处理视频;在相邻帧中,同一个 landmark index 可能沿 contour 发生微小滑移或交换,导致轨迹抖动。困难点在于:单帧 mask 监督对这种时间错位几乎不可见,因为每帧边界仍然可以贴合得很好;但临床下游如 EF、wall motion、regional strain 依赖的是连续轨迹而非独立 mask。以前 pixel segmentation 没有 landmark identity,post-hoc optical flow/Kalman/autoencoder smoothing 又和分割模型解耦,无法把 anatomical correspondence 作为优化对象。关键矛盾是空间拟合目标允许多解,而 temporal clinical measurement 要求解在时间上唯一且稳定。
Motivation
已有路线不够的地方不是分割边界不够准,而是 representation 不适合时间分析。pixel mask 的拓扑和区域语义是后验解释出来的;registration/optical-flow 可以估计运动,但通常不保证和 segmentation model 内部的解剖索引一致;post-processing 可以变平滑,却未必恢复正确 anatomical identity。作者看到的缺口是:既然 landmark model 已经拥有固定节点索引,那么视频本身可以提供额外监督信号——同一节点在时间上应该走一条生理合理的轨迹。这个方向自然来自一个很直接的观察:cardiac ultrasound 的标注稀缺集中在 ED/ES,但完整视频很容易获得,因此 temporal coherence 是一种可利用的 self-supervision。
Core Idea
核心思想是把 learned anatomical correspondence 从“跨个体静态对齐”扩展为“跨时间动态对齐”。基础模型先通过 mask-level supervision 学出固定图结构和 landmark index;随后在未逐帧标注的视频上,对每个 index 的 velocity 和 acceleration 加惩罚,使模型倾向于输出平滑轨迹。这样做的本质不是加一个 smoothing module,而是改变训练约束:同一 landmark 的时间一致性成为模型参数的一部分,而不是输出之后的修补。
这个方法引入的 inductive bias 是 cardiac anatomy 的低频运动先验。它假设 speckle、边界模糊和 Chamfer 多解会产生高频 jitter,而真实心肌运动在相邻帧上应当速度/加速度连续。和 prior 的本质区别在于它依赖 landmark identity 来定义 temporal loss;没有这一点,速度/加速度 loss 只是在任意点集或 mask 上做平滑,语义弱很多。scalability 来自不需要逐帧标签,只需要视频序列;但 generalization 的上限也被这个强运动先验限制。
Method
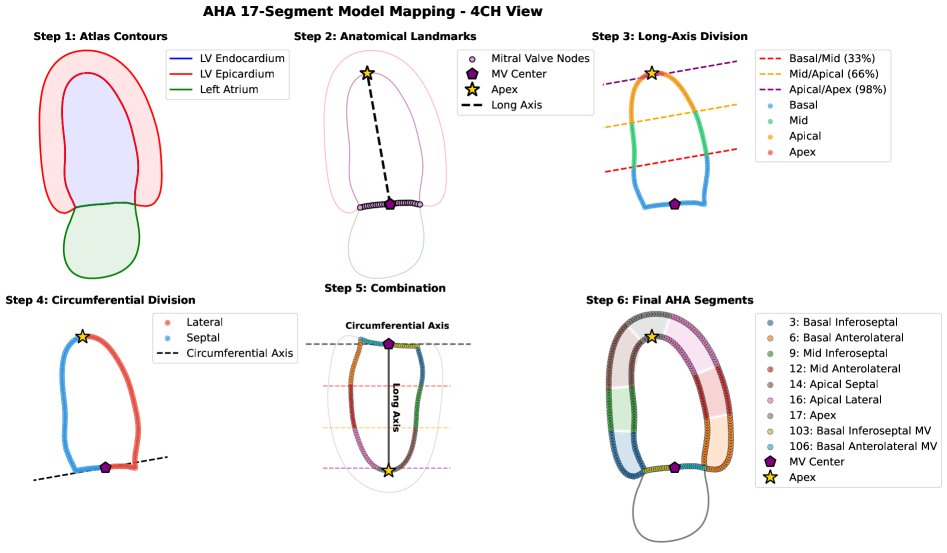
方法的必要机制可以压缩为四点。第一,固定拓扑 landmark graph 提供可微、可追踪的解剖索引,这是 temporal regularization 能有语义的前提;如果 index 不稳定,平滑的是错误对象。第二,base loss 仍然保留 Chamfer、shape regularization、pixel Dice/VAE 等空间约束,用来保证 contour 不因时间平滑而漂离真实 anatomy。第三,velocity loss 压制 frame-to-frame displacement 中的高频成分,主要针对 landmark 沿 contour 的跳点和 ultrasound noise 诱导的抖动。第四,acceleration loss 比单纯速度惩罚更重要,因为心脏收缩/舒张本来有位移,不能把运动整体压小;二阶平滑更接近“允许运动,但不允许运动模式突变”。交替训练 annotated frames 与 unlabeled sequences 的意义是防止 temporal loss 的退化解,即预测几乎静止但很平滑的轮廓。AHA mapping 不是核心优化贡献,而是把 correspondence 变成 clinical regional readout 的桥:在平均 atlas 上一次性确定 segment assignment,再把该 assignment 复制到每个病例的节点轨迹。
Key Insight / Why It Works
最关键的 insight 是:在 landmark-based segmentation 中,时间一致性只有在 node identity 已经有解剖语义时才是强约束;否则它只是普通平滑。论文的贡献主要不是 velocity/acceleration loss 本身——这是经典 trajectory smoothing——而是把它放在 implicit correspondence graph 的后训练阶段,使 temporal smoothness 约束的是“同一 anatomical landmark 的运动”,而不是 mask boundary 的任意点。
它有效的原因很可能有三层。第一,Chamfer distance 对点顺序不敏感,容易留下沿 contour 的 index oscillation;temporal loss 正好补上这个不可辨识性。第二,ultrasound 单帧外观噪声高,时间上的低频运动先验能在多个空间可行解中提供选择压力。第三,post-training 而不是 joint-from-scratch 让 correspondence 先成形,再做轨迹校准,这更像 curriculum / representation alignment,而不是端到端新架构。
我认为核心贡献是 representation-level temporal regularization;AHA mapping 是有价值的应用包装,但技术上更多是利用已有 correspondence 的 deterministic clinical mapping。增益来源不清的一点是:论文没有充分隔离“模型内部 fine-tuning”与“输出轨迹后处理滤波”的差异;如果大部分 improvement 来自低通滤波效应,那么方法的新颖性会弱一些。另一个风险是 temporal smoothness 可能把真实病理运动也压平,尤其是 regional dyssynchrony 或局部运动异常;文中展示其可检测 hypokinesis/dyssynchrony,但没有足够证据证明正则不会损伤这些信号。
Relation To Prior Work
这篇工作最接近三条线:HybridGNet/Mask-HybridGNet 的 graph-based anatomical segmentation,echocardiography temporal consistency/post-processing,以及传统 registration/optical-flow cardiac motion estimation。它不是从零提出新的 cardiac motion model,而是在 Mask-HybridGNet 的 implicit correspondence 上增加 temporal self-supervised refinement。
和 PDM/ASM/HybridGNet 的差异在于它不依赖人工 landmark correspondence,而是继承 mask-supervised emergent correspondence;和 nnUNet/pixel segmentation 的差异在于输出天然是可追踪节点而非无身份 mask;和 Kalman/optical-flow/autoencoder post-processing 的差异在于 temporal constraint 回传进 segmentation model,而不是只修输出。看似新的 velocity/acceleration 正则其实是老思想,实质创新在于它被施加在 anatomical-indexed graph decoder 的输出空间,并与空间监督交替保持。技术谱系上,它属于 structured-output segmentation + self-supervised temporal consistency + clinical atlas mapping 的组合,而不是纯 segmentation architecture paper。
Dataset / Evaluation
评估集中在 CAMUS:500 个 2CH/4CH echo 序列,ED/ES 有标注,视频约 20 帧。这很适合验证作者 claim 的核心场景:标签稀疏但视频连续,且临床指标依赖 LV volume 和 motion。实验覆盖了 spatial metrics、clinical metrics 和 trajectory metrics,因此比只报 Dice 更贴近论文主张。
但 evaluation 的外推性有限。它没有真正证明跨医院、跨设备、跨帧率、跨病种泛化,也没有真实部署中的 tracking failure analysis。temporal metrics 如 jitter/FTD/jerk 与训练 loss 高度同构,容易偏向正则化模型;它们能说明轨迹更平滑,但不等价于真实运动更准确。nnUNet + mask-to-landmark post-processing 是合理对照,但这个 post-processing 模型本身可能不是最强的 trajectory extraction baseline。整体看,实验支持“在 CAMUS 上 temporal regularization 让 landmark trajectories 更平滑且不明显牺牲分割”,但不足以支持“可靠检测病理区域运动模式”的强临床 claim。
Limitation
最大限制是方法把 correspondence correctness 当成前提。如果基础模型学到的 landmark index 已经错位,temporal regularization 只会稳定错误 correspondence。第二,smooth motion prior 不总是临床正确:病理性不同步、局部低运动、瓣膜平面附近复杂运动、out-of-plane motion 都可能被过度平滑。第三,AHA mapping 依赖平均 atlas、长轴定义和标准视图几何;异常形态、成像切面偏移、LA/LV shared node 识别错误都会把 regional analysis 系统性带偏。
scalability 上,完整序列反传受显存限制,论文也承认 T 受限;更长序列、更高帧率或多周期数据未验证。泛化是否真实存在文中未充分说明,因为只在 CAMUS 上验证,且 CAMUS 的 ED/ES 标注和标准采集条件比较规整。增益归因不清:可能一部分只是 model-internal smoothing / low-pass filtering,而不是更好的 motion understanding。方法也把问题从“逐帧分割不稳定”转移成“如何选择不会抹掉病理信号的 temporal prior”,这个 trade-off 需要更严格的临床运动 ground truth 才能判断。
Takeaway
- 最值得记住的是:对于 cardiac segmentation,空间准确性和轨迹可用性是两个不同目标,Dice 高不代表能做 regional motion analysis。
- 第二,landmark correspondence 的价值不只在 topology guarantee,还在于它提供了定义 self-supervised temporal loss 的坐标系;这是 pixel mask 很难直接拥有的。
- 第三,这篇论文真正推动的是把 anatomical correspondence 从静态 population analysis 推向 temporal clinical measurement,而不是提出复杂新架构。
- 第四,未来更值得做的是用真实 motion/strain reference、跨设备数据和病理分层来验证 temporal prior 是否保真,而不是继续只优化平滑指标。
一句话总结
这篇论文是 Mask-HybridGNet 式 anatomical-correspondence segmentation 向 temporally coherent clinical motion analysis 的自然延伸,真正贡献在于把视频时间连续性作为自监督约束施加到有解剖身份的 landmark graph 上,而不是单纯做更强分割或后处理平滑。