精读笔记
Problem Setting
这篇论文的真实 problem setting 是 cardiac digital twin pipeline 中的 simulation-ready volumetric mesh reconstruction,而不是常规 surface mesh reconstruction。关键矛盾是:simulation 需要高质量 tetrahedra、跨病例一致连接和可控 element specification;医学图像边界又存在薄壁、multi-structure junction、partial-volume 等局部不确定性。传统 segmentation-then-meshing 可以靠局部几何贴合目标,但 TetGen/后处理会产生 case-dependent sampling/connectivity;deformation-based image-to-mesh 可以保 topology 和 correspondence,但通常停在 surface,且 deterministic Chamfer/L2 监督会在不确定边界处产生过平滑或错配。论文试图同时保住 correspondence、boundary fidelity 和 volumetric usability,但它选择的路线不是学一个端到端 tetrahedral generator,而是把可学习部分集中在 surface deformation,再用 template warping 继承体网格质量。
Motivation
已有路线缺的不是一个更大的 3D CNN,而是合适的 representation alignment:图像中的边界不确定性是方向相关的,而 mesh loss 通常把所有方向误差等价处理;simulation mesh 需要体连接一致,而 surface-only 方法后接 tetrahedralization 会破坏 correspondence。作者的核心观察是,心脏多结构边界处的“正确监督”不应只是把 vertex 拉到最近点,而应允许不同方向上的局部容差被显式建模。同时,真正可部署的 in-silico pipeline 往往重视 mesh specification 的可控性,因此固定 template 的工程优势很大。换言之,论文动机是把 learning 用在最需要统计建模的表面定位,把 meshing 留给可控的 template-conditioned deformation。
Core Idea
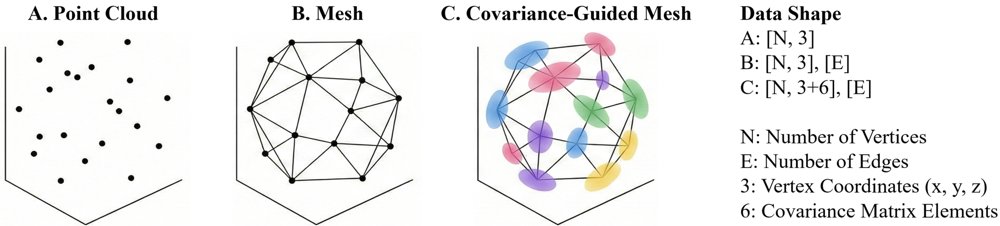
核心思想可以概括为:surface reconstruction 用 probabilistic local metric,volumetric reconstruction 用 deterministic template transport。前者把每个 template vertex 建模为 anisotropic Gaussian kernel,网络不仅预测 mean displacement,也预测 SPD covariance;训练时用 Mahalanobis term 加 log-det penalty,使匹配误差在局部 learned metric 下计算。这样模型不再被迫在边界模糊方向上做硬点估计,而是能学习到方向性容差,从而更适合薄壁和交界区域。
后者的本质是把 tetrahedral meshing 从生成问题改写成变形传播问题:只要固定 template 的体连接和 element quality 足够好,预测 surface 之后通过 global alignment、non-rigid registration 和 deformation-field propagation 把整个体网格带过去,cross-case correspondence 就由 template connectivity 自动保证。这和 prior 的差异不在于用了 CNN-GNN 或 registration 本身,而在于它把 uncertainty-aware surface learning 与 correspondence-preserving volume transport 组合成一个面向 simulation 的表示链条。
Method
方法层面最关键的是三个机制。第一,covariance-guided graph deformation 解决 deterministic vertex supervision 对边界不确定性建模不足的问题;它的核心变化是从 isotropic Euclidean geometry 切换到 per-vertex anisotropic metric,使 vertex matching 带有方向性置信度。第二,Cholesky-parameterized covariance 不是主要创新,但它是让 NLL 可训练、SPD 稳定和 log-det penalty 可用的必要工程约束;没有它 covariance 很容易退化成不可逆或无限膨胀。第三,template-driven volumetric warping 解决的是体网格 correspondence 和 element specification 控制问题;它不学习 tetrahedral connectivity,而是复用 template connectivity,再通过 surface-to-volume deformation field 把表面运动传播到内部。mesh regularization 的角色更像防止 learned surface deformation 破坏后续 volume warp 的安全带,而不是主要性能来源。
Key Insight / Why It Works
最可能真正有效的部分是 representation alignment:医学边界的不确定性和 mesh supervision 的几何度量终于对齐了。Chamfer/L2 把 nearest-neighbor matching 视为确定事实,但在 atrial myocardium、ventricular junction、thin wall 这些区域,GT mesh 本身可能来自 segmentation/post-processing,局部边界并非精确点标签。Anisotropic covariance 相当于给每个 vertex 学一个局部误差椭球,既能降低 ambiguous direction 的过惩罚,又能在可靠方向保持约束,因此会改善 HD95/CD 和 normal consistency。
第二个有效原因是它强烈利用了 template prior。所谓 volumetric reconstruction 的泛化,很大程度上来自固定 tetrahedral template 的 memory reuse:连接关系、element distribution、结构语义都预先编码在 template 里,网络只需要预测一个相对低维的 deformation。这个 inductive bias 对心脏这种 topology 相对稳定的器官非常合理,但它不是通用 3D meshing 能力。
第三,体网格质量的提升不应完全归功于 learning。0 inverted elements、较好的 Jacobian/dihedral 很可能主要来自 template quality + smooth deformation propagation + regularization,而非 covariance 本身。covariance 主要改善 surface boundary localization;volume mesh quality 主要由 template 和 registration pipeline 决定。论文把两者都放在 HeartVolMesh 下是合理系统设计,但技术归因需要拆开看。
需要警惕 hidden supervision / evaluation bias:reference pseudo-GT mesh 的生成过程包含同类 template-warping procedure,而方法最终也使用 template-conditioned warping;这可能让评估天然偏向 template-deformable solutions。增益不一定是 benchmark leakage,但“与 pseudo-GT representation 对齐”很可能贡献了不少。
Relation To Prior Work
这篇最接近 Voxel2Mesh / MeshDeformNet / HeartDeformNet 这条 template deformation image-to-mesh 谱系,而不是传统 tetrahedral meshing 或 implicit neural representation。和这些 prior 的本质差异有两个:一是 supervision 从 deterministic Chamfer-style matching 变成 covariance-aware NLL,给每个 vertex 引入 learned anisotropic uncertainty;二是目标从 surface mesh 扩展到 template-corresponded tetrahedral volume mesh。
看似新的部分中,CNN encoder、GNN deformation、coarse-to-fine unpooling、edge/Laplacian/normal regularization 都是已有思想重组;Cholesky covariance 和 uncertainty-weighted loss 也可追溯到 heteroscedastic uncertainty learning。实质创新在于把这些思想放到 cardiac image-to-mesh 的 vertex-level geometric supervision 中,并且与 template tetrahedral warping 组合,形成一个 simulation-oriented pipeline。它不是端到端 mesh generation 的新范式,更像是 deformation-based medical mesh reconstruction 的 probabilistic-supervision + template-transport 版本。
Dataset / Evaluation
评估覆盖了 whole-heart / multi-structure 场景,并且数据规模对医学 mesh 任务来说不小:multi-centre in-house,patient-level split,包含 temporal instances。它足以支持作者在该数据分布内的 surface/volumetric boundary accuracy claim,也能说明 covariance-guided supervision 相比 Chamfer-only 有稳定收益。
但 evaluation 没有完全验证论文更强的 deployment claim。首先,数据和 pseudo-GT 都是内部流程生成,缺少公开 benchmark 和外部协议验证;其次,reference mesh 来自 TotalSegmentator + manual refinement + template-warping,这会让“template-preserving reconstruction”在 representation 上占便宜;第三,volumetric mesh 主要通过 boundary surface metrics 和 element-quality statistics 评估,没有真正跑 downstream FEM/CFD,看不到 solver stability、物理量误差或 clinical endpoint 影响。换言之,实验验证了几何层面的 pipeline plausibility,但还没有验证 simulation-readiness 的完整闭环。
Limitation
方法成立依赖几个强前提。第一,目标 anatomy 必须和 template 同拓扑且形变幅度在 registration 可承受范围内;复杂先天畸形、术后结构、拓扑变化或极端病理可能直接突破 template prior。第二,cross-case correspondence 是 construction property,但不自动等于 anatomical correspondence;如果 template-to-patient deformation 在某些区域发生滑移,顶点编号一致也可能只是形式一致。第三,covariance 的可解释性文中未充分说明:它可能学到真实边界不确定性,也可能只是 loss attenuation 或 outlier masking。
scalability 上限主要由 template density、deformation field resolution、registration stability 和 GPU memory 决定。作者说 resolution controlled by template density 是优点,但高密度 template 下 registration/field propagation 的计算和质量控制会成为新瓶颈。另一个问题是增益来源不清:Ours3p6 相比 Ours3p1 的收益被解释为 anisotropic covariance modelling,但是否同时包含更多参数、更细表示或其他 scaling factor,文中信息不足。最后,所谓 volumetric meshing capability 实质上是 high-quality template reuse,不是从图像中学习生成任意质量 tetrahedralization;这不是缺点,但边界应说清楚。
Takeaway
- 最值得记住的不是“用 covariance 预测 mesh”,而是 medical mesh learning 中 loss geometry 需要匹配 annotation uncertainty:边界模糊不是噪声,而是方向相关的监督结构。
- 第二,simulation-oriented mesh reconstruction 可能不应追求纯端到端;template-conditioned design 在需要 correspondence、element quality 和 mesh specification 控制时更实际。
- 第三,这篇推动的是 image-to-surface learning 与 volume mesh transport 的系统整合,而不是通用 tetrahedral meshing。
- 未来真正值得做的是:验证 covariance 是否可校准,比较不同 template specifications 的上限,把 evaluation 从 geometric metrics 推到 solver-level quantities,并测试跨模态/跨病理/跨机构的 failure mode。
一句话总结
HeartVolMesh 是 deformation-based cardiac image-to-mesh 路线向 simulation-ready volumetric meshes 的一次务实演化:用 learned anisotropic uncertainty 改善表面监督,再用固定 tetrahedral template transport 换取跨病例体网格 correspondence 和可控 mesh quality。